1 Human Engineering Research Laboratories, Department of Veterans Affairs, Pittsburgh, PA
2 Department of Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA
3 Department of Biomedical Engineering, Marquette University, Milwaukee, WI
ABSTRACT
The purpose of this study was to perform a systematic literature review to find relevant scientific articles concerning the performance of independent transfers from a wheeled mobility device to/from another surface. This is the first phase of a project funded by the US Access Board which aims to improve the accessibility guidelines for recreational facilities such as amusement parks. Forty-two articles were formally reviewed and scored by twelve experts. Ten articles were determined to be at least moderately relevant to the topic based on the score in relevancy of the research topic. There is a consensus among studies that transferring to a higher surface implies greater exertion of the upper limb. However, there is no evidence about the ranges, location of the wheelchair in space, use of supports, use of a transfer board, and gap between wheelchair and target surface.
KEYWORDS
Independent transfers; literature review; wheeled mobility devices.
BACKGROUND
For individuals who rely on wheeled mobility devices, performing transfers is essential to achieving independence with activities of daily living (ADL) inside and outside the home. For example, transfers are required for getting to and from the device to bed, bath tub/shower seat, commode seat, motor vehicle seat and so on. Long standing accessibility standards have established the desirable height and position of clear space for a limited number of elements where transfer is expected. Additional guidance is needed for transferring to elements that may require more than one transfer; vertical transfer up to or down into a new position; transfer where space for positioning one’s mobility device is limited; and transfers into confined spaces.
Within the scientific community there has been a recent surge of interest in investigating wheelchair transfers for the purposes of understanding the etiology of upper limb pain and injury which is highly prevalent among wheelchair users and to identify methods of transfer that are more efficient and safer for individuals (1 ), (2 ), (3 )]. The purpose of this study was to conduct a systematic literature review to identify current state of the science on various issues concerning independent transfers primarily related to setup and assistive device use. Results from the study will be used to help define optimal design characteristics for transfer surfaces that have the least negative impact for wheeled mobility devices users.
METHODOLOGY
Literature Review Process
Scientific and medical databases were searched using Scopus (1966 to 2009), OVID Medline® (1950 to 2009), Compendex (1969 to 2009), and EMBASE (1974 to 2009). Keywords used in this literature review in alphabetical order were: wheelchair + activities of daily living; biomechanics; efficiency; electromyographic; force; force plate; function; functional electrical stimulation; gait; isokinetic; kinematics; kinetics; measurement system; moment; motion analysis; movement; muscle balance; muscular demand; orthosis; paralysis; paraplegia; rehabilitation; scapula; shoulder; SCI; stroke; SCI patient; shoulder impingement; standing up; task performance and analysis; technology; tetraplegia; torque; torque ratio; transfer; transfer motion; transfer strategy; transfer movement strategies; upper extremity; upper limb; weight-bearing; weight bearing; three dimensional kinematics. Three-hundred and thirty-nine articles (excluding duplicates) were initially identified by keyword search, followed by backward searching and finishing with forward searching (4 ).
Expert Review and Scoring Procedures
Titles and abstracts of the articles were reviewed internally by three internal experts. Forty-one articles were determined to be related to the performance of independent transfers. Only peer-reviewed scientific full journal articles were included in this review. Following this preliminary internal review, twelve external reviewers who are collaborators, researchers and/or practitioners in assistive technology and/or the rehabilitation field were asked to score the forty-one articles using a scoring sheet for each article (Figure 1). For question number one, if a reviewer responded that they have no expertise to evaluate the article, the reviewer did not complete the subsequent questions and was instructed to proceed to the next article. As a result, when an article was not reviewed, his/her data were not considered when calculating the mean score for the questions in that article. Questions number two and three were scored zero- not relevant to three- highly relevant. Question number four was scored five- Systematic review or meta-analysis of randomized trials, zero- Case study, nonsystematic review, or similar very weak design, based on the Spinal Cord Medicine Clinical Practice Guideline (5 ). Finally, the strength of the resulting evidence was scored in zero- weak resulting conclusions and 3- very strong resulting conclusions.
Data Analysis
The first cut-off criterion was based on the relevance question; only articles with a mean relevance score across reviewers greater than or equal to 1.1 were included. The second cut-off criterion was based on the strength of the resulting evidence; only articles with a mean strength score greater than or equal to 1.1 were included. After selecting the articles that were relevant and strong enough, the top ten scored ones were selected for discussion.
RESULTS
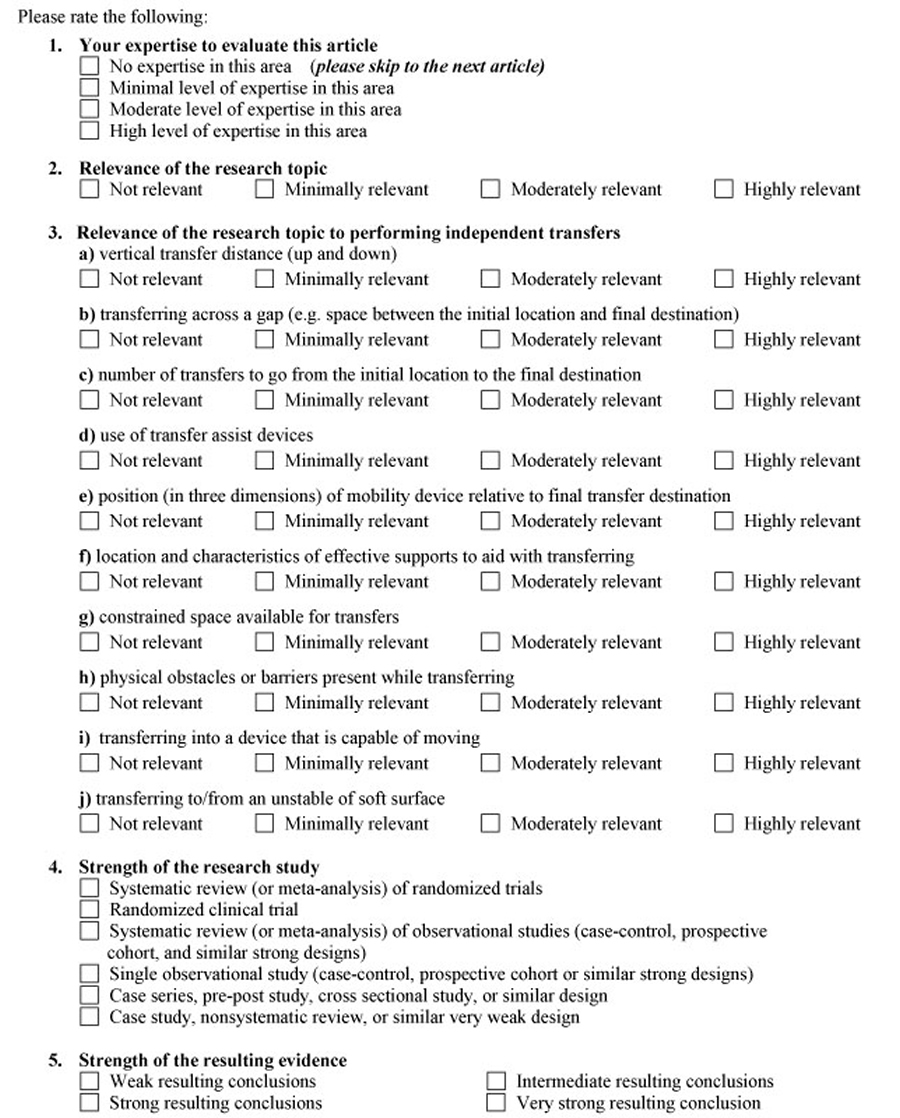 Figure 1.
Figure 1.Forty articles out of forty one were scored greater or equal than 1.1 for the relevancy of the research topic. From these articles, twenty six were scored greater than or equal to 1.1 in the strength of the resulting evidence. For the purpose of this paper, the top ten scored articles based on relevancy were selected for discussion. These papers were all rated as ‘moderately relevant’ to the topic. All of these articles scored greater or equal than 1.1 for the items vertical transfer distance and transferring across gap. Seven scored greater or equal than 1.1 for the item position (in three dimensions) of mobility device relative to final transfer destination. Three scored greater or equal than 1.1 for the item number of transfers to go from the initial location to the final destination. Only one article scored greater or equal than 1.1 for the item location and characteristics of effective supports to aid with transferring, constrained space available for transfers, and physical obstacles or barriers present while transferring. None of the articles scored greater or equal than 1.1 for the item transferring to/from an unstable of soft surface. Table 1 presents the scores obtained for the top ten scored articles. All other studies are listed in Table 2.
Nyland, et al (6 ) performed a literature review that described the use of the upper extremity for transfers among people with spinal cord injuries and factors associated with upper extremity joint degeneration and loss of transfer independence. They reported a Wang, et al (7 ) study that concluded that equal wheelchair seat and target transfer surface heights enabled subjects to perform transfers with considerably less upper extremity muscular effort.
Six of the ten studies were by Gagnon et al [(8 ),(9 ),(10 ),(11 ),(12 ),(14 )] who studied the biomechanics and muscular demand of performing sitting pivot transfers in small groups of SCI in different target surface height [(8 ),(9 ),(11 )], posterior transfers in SCI in two studies [(10 ),(14 )], and a comparison between weight relief and transfer maneuver (12 ). Findings in the pivot transfer studies included that lowering the target seat with respect to the initial seat had no favorable effect on muscular demand (8 ). The results showed maximum shoulder flexion and excursion of the trailing upper extremity amplified as target seat height increased (9 ). For the trailing hand, higher mean vertical reaction force was recorded when transferring toward the high target seat and vice-versa for the leading hand that reached a greater mean vertical reaction force when transferring to the target seat of the same height (11 ). The trailing hand supported additional vertical reaction force when transferring to the high seat compared with the one of same height (11 ). For the elbow, additional extension was required at the leading elbow when transferring to the low or high target seat compared to one of similar height (9 ). Limitations of all of these studies include fixed angles between the seats, which may differ from the setup subjects use regularly to perform transfers [(8 ),(9 ),(11 ),(12 )]. Regarding posterior transfers, the results suggested that transferring backwards to a higher surface did not require a greater amount of muscular demand than did the transfer on the even surface (14 ). The firmness of the transferring surface could influence the movement and muscular strategies (10 ). By comparing single pivot with weight relief maneuver, they concluded that single pivot transfers can be ranked as one of the most mechanically demanding routinely performed wheelchair related activity among individuals with SCI (12 ).
Nawoczenski, et al (13 ) studied three-dimensional scapulothoracic and glenohumeral kinematics in twenty-five able-bodied subjects during weight-relief lift and while transferring to/from a wheelchair to a surface of equal height. There were significant differences for transfer direction for scapular downward and upward rotation (P<0.01), as well as for scapular internal and external rotation across phases and transfer directions (both P<0.01). However, this study was performed on able-bodied subjects so it could not be generalized to people with SCI.
Finley, et al (15 ) studied twenty-three male manual wheelchair users- thirteen without shoulder impingement and ten with impingement. Two benches were placed at a 45° angle to each other at the height of the individual subject’s wheelchair. Subjects transferred from one bench to the other bench, first towards the dominant (lead limb transfer), then returning towards the non-dominant (trail limb transfer). Manual wheelchair users with impingement had increased scapular upward rotation at 31 degrees (P=0.01). The trail limb transfer had reduced scapular axial rotation excursion (P<0.01) as compared with the lead limb transfer.
Perry, et al (16 ) recruited twelve adult men with SCI to evaluate the intensity of selected shoulder muscle activity during depression transfers using intramuscular electrodes to record the activity. Transfer maneuver required more muscular strength than weight-relief maneuver.
DISCUSSION
This paper reflects the expert reviewers’ perception of the relevancy and strength of current evidence on the performance of independent transfers. Our study revealed a very small number of studies that direct relate to the influence of transfer setup on performing independent transfers and thus points to a critical need for more studies in this area. Despite finding articles that were moderately relevant, the strength of the evidence was generally considered to be low (< 2) calling for stronger research designs to be employed for the future studies on transfers. All the studies identified also involved small groups of subjects and subjects with SCI or unimpaired subjects which may not be generalizable to other populations who do independent transfers.
There is a consensus among studies that transferring to a higher surface implies greater exertion of the upper limb [(8 ),(9 ),(11 ),(14 )]. However, there have not been studies that have specifically investigated the range of heights feasibly attainable by subjects which is important for determining the suitability of existing accessibility guidelines concerning transfers (ADAAG, Section 15, (17 )).
The elements of transfer setup concerning wheelchair space and orientation differed across studies [(8 ), (9 ), (11 ), (12 ), (15 )], and thus it remains unknown how these attributes affect the transfer.
Our study highlights the need for future studies particularly as it relates to the interaction between distance from the wheeled mobility device, space available to place and maneuver the mobility device, availability of supports (i.e. grab bars), number of the transfers to go from the initial location to the final destination, use of transfer assistive device, constrained space available for transfers, physical obstacles or barriers present while transferring, transferring into a device that is capable of moving, and transferring to/from an unstable of soft surface.
REFERENCES
- Gagnon D, Koontz AM, Mulroy S, Nawoczenski D, Butler-Forslund E, Granstrom A, Nadeau S, Boninger ML. Biomechanics of sitting pivot transfers among individuals with SCI: A review of the current knowledge. Topics in SCI Rehabilitation, in press.
- Kankipati P, Koontz AM, Turkovich M. (2008). Shoulder joint loading for three types of lateral wheelchair transfers. Proceedings of the RESNA Annual Conference, Arlington, VA, June 26-30, CD-ROM
- Kankipati P, Koontz AM, Boninger ML, Lin Y. (2009). Hand and shoulder joint kinetic analysis of three types of lateral wheelchair transfers. Proceedings of the RESNA 2009 Annual Conference, New Orleans, LA, June 23-27, CD-ROM
- Levy Y, Ellis TJ. (2006). A systems Approach to Conduct an Effective Literature Review in Support of Information Systems Research. Informing Science Journal Volume 9.
- Consortium for Spinal Cord Medicine. (2005). Preservation of upper limb function following SCI: a clinical practice guideline for health-care professionals. Washington (DC): Paralyzed Veterans of America
- Nyland J, Quigley P, Huang C, Lloyd J, Harrow J, Nelson A. (2000). Preserving transfer independence among individuals with SCI. (Review) (70 refs). Spinal Cord Nov;38(11):649-57.
- Wang Y et al. (1994). Reaction force and EMG analyses of wheelchair transfers. Percep Mot Skills79: 763-766.
- Gagnon D, Nadeau S, Noreau L, Eng JJ, Gravel D. (2009). Electromyographic patterns of upper extremity muscles during sitting pivot transfers performed by individuals with SCI. Journal of Electromyography and Kinesiology June 19(3), 509-520. 12
- Gagnon D, Nadeau S, Noreau L, Eng JJ, Gravel D. (2008). Trunk and upper extremity kinematics during sitting pivot transfers performed by individuals with SCI. Clinical Biomechanics (Bristol, Avon) March 23(3), 279-290. 9
- Gagnon D, Nadeau S, Gravel D, Noreau L, Lariviere C, Gagnon D. (2003). Biomechanical analysis of a posterior transfer maneuver on a level surface in individuals with high and low-level spinal cord injuries. Clinical Biomechanics (Bristol, Avon) May 18(4), 319-331. 7
- Gagnon D, Nadeau S, Noreau L, Dehail P, Gravel D. (2008). Quantification of reaction forces during sitting pivot transfers performed by individuals with SCI. Journal of Rehabilitation Medicine June 40(6), 468-476. 11
- Gagnon D, Nadeau S, Noreau L, Dehail P, Piotte F. (2008). Comparison of peak shoulder and elbow mechanical loads during weight-relief lifts and sitting pivot transfers among manual wheelchair users with SCI Journal of Rehabilitative Research and Development 45(6), 863-873. 14
- Nawoczenski DA, Clobes SM, Gore SL, Neu JL, Olsen JE, Borstad JD, Ludewig PM. (2003). Three-dimensional shoulder kinematics during a pressure relief technique and wheelchair transfer. Archives of Physical Medicine and Rehabilitation September 84(9), 1293-300. 8
- Gagnon D, Nadeau S, Gavel D, Noreau L, Lariviere C, McFadyen B. (2005). Movement patterns and muscular demands during posterior transfers toward an elevated surface in individuals with SCI. Spinal Cord February 43(2), 74-84. 13
- Finley MA, McQuade KJ, Rodgers MM. (2005). Scapular kinematics during transfers in manual wheelchair users with and without shoulder impingement. Clinical Biomechanics (Bristol, Avon) January 20(1), 32-40. 15
- Perry J, Gronley JK, Newsam CJ, Reyes ML, Mulroy SJ. (1996). Electromyographic analysis of the shoulder muscles during depression transfers in subjects with low-level paraplegia. Archives of Physical Medicine and Rehabilitation April 77(4), 350-355. 10
- US Access Board. (2002). ADA Accessibility Guidelines for Buildings and Facilities (ADAAG). Available from http://www.access-board.gov/adaag/html/adaag.htm
ACKNOWLEDGEMENTS
Funding for this study was provided by the Department of Education (NIDRR), United States Access Board grant H133E070024 and Project #84.133E.
Author Contact Information:
Maria L. Toro BS, University of Pittsburgh, Human Engineering Research Laboratories, Pittsburgh, PA, 15206, Office Phone (412) 954-5302, EMAIL: mlt47@pitt.edu